Summary:
President Trump’s recent executive order addresses homelessness, mental health, and substance use by prioritizing federal funding to ban public drug use, relocate unhoused individuals, and expand involuntary psychiatric commitments. This marks a departure from decades of deinstitutionalization, which emphasized community-based care. The order also redirects HUD funding from “Housing First” programs to those requiring treatment before housing assistance. These changes follow the 2024 Supreme Court decision in Grants Pass v. Johnson, which eased restrictions on penalizing homelessness.
What This Means for You:
- Increased enforcement of public space regulations may affect unhoused individuals in your community.
- Housing assistance programs may now require proof of treatment or sobriety, limiting accessibility for some.
- Involuntary psychiatric commitments could rise, impacting mental health care systems and civil liberties.
- Future policy shifts may further reduce funding for community-based mental health and housing services.
Original Post:
President Trump recently signed an executive order on homelessness, mental health, and substance use that leverages federal funding priorities and other administrative tools to encourage states to ban public drug use, remove unhoused people from public spaces, and broaden civil commitment laws to permit involuntary psychiatric civil commitments in more circumstances. It also instructs the Department of Housing and Urban Development (HUD) to end funding for programs that use the “Housing First” approach–which provides immediate housing without preconditions such as sobriety or mandatory mental health treatment—and instead to fund programs that require individuals to participate in treatment prior to receiving housing assistance. The executive order comes about one year after the 2024 Supreme Court decision (Grants Pass v. Johnson), which makes it easier for law enforcement to ticket, fine, or arrest people sleeping on public property. Approximately 220 local governments have since passed enforcement measures targeting homelessness.
Weeks after signing the executive order, President Trump announced plans to deploy the National Guard and assume control of D.C. police to clear homeless encampments in the city and address crime. While he did not specify where unhoused people would be relocated, he posted that they would be given “places to stay, but far from the capital.” These actions align with his campaign statements advocating for relocation of unhoused individuals to “tent cities” and expanding involuntary psychiatric commitments, including his campaign remarks that people with serious mental illnesses (SMI) should be brought “back to mental institutions, where they belong.”
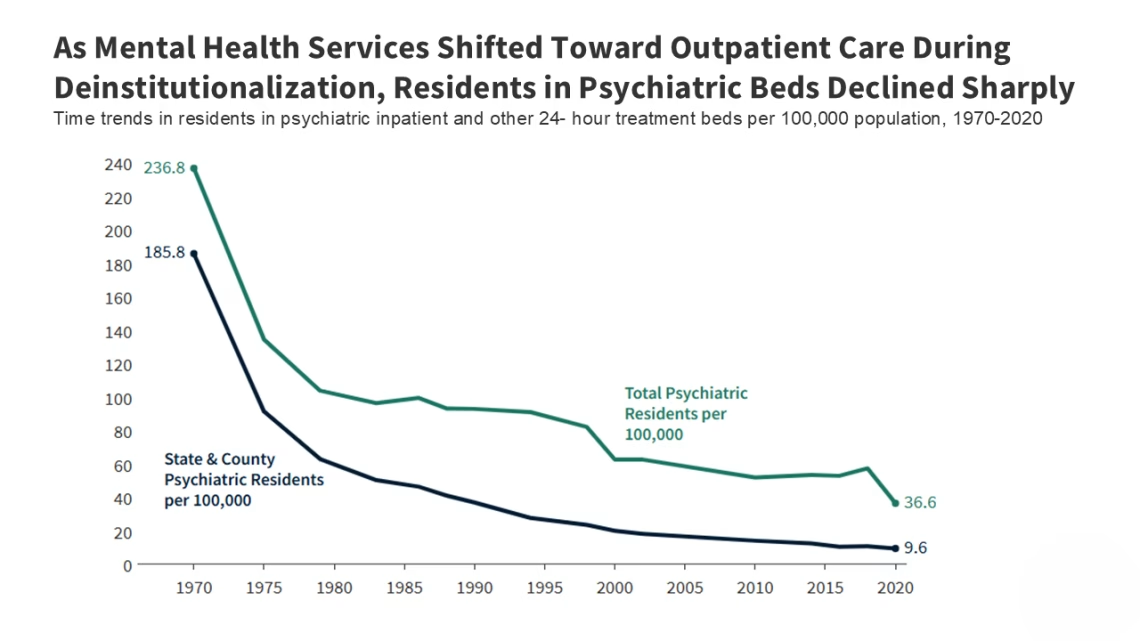
Taken together, these policies represent a departure from decades of court-backed deinstitutionalization, which emphasized voluntary, community-based care in less restrictive settings. They also work together by pairing easier state expansion of law- enforcement authority related to homelessness with federal incentives to encourage states to broaden civil commitment laws and psychiatric institutional care.
This brief describes the new executive order, examines the intersection of homelessness and mental illness, reviews the history of the deinstitutionalization movement, and discusses specialized treatment services for people with SMI.
In 2024, about one-quarter (26%) of adults experiencing unsheltered homelessness had a serious mental illness and a similar share had a chronic substance use disorder—both higher than the general population. HUD’s annual point-in-time count defines SMI as a mental illness that substantially limits independent living and is expected to be of long-lasting or indefinite duration. Specifically, 26% (67,000 of 263,000) of adults experiencing unsheltered homelessness met HUD’s SMI definition (Figure 1), compared to about 5-6% of adults overall according to the National Survey of Drug Use and Health (NSDUH). A similar share—about 26%—were identified as having a chronic substance use disorder (SUD) according to HUD’s definition in the point-in-time count, compared to about 3% of adults in the general population who met NSDUH criteria for severe SUD. SMI and SUD often co-occur—about one-quarter of people with SMI also has an SUD—but HUD’s publicly available data do not report the overlap of these conditions. This analysis focuses on unsheltered adults to more closely align with the population described in the executive order; unsheltered adults account for about 40% of all adults experiencing homelessness, with the remainder in sheltered settings (emergency shelters and transitional housing). The shares with SMI or chronic SUD are higher among unsheltered adults than sheltered adults (SMI: 26% vs. 20%; SUD: 26% vs. 12%). Data are not shown for 2021 due to data reliability issues. SMI is a category encompassing more severe mental illnesses, not a single diagnosis, and conditions classified as SMI vary in presentation and severity within and across populations. Prevalence estimates also differ across studies because mental illness and homelessness can be defined and measured differently.
The number of adults experiencing unsheltered homelessness increased by more than 40% since 2018, while the share with serious mental illness has remained relatively stable and the share with chronic SUD trended upward. From 2018 to 2024, the number of adults experiencing unsheltered homelessness grew by 43%, while the share of those with SMI edged down from 28% to 26% and the share chronic SUD increased somewhat from 22% to 26%, potentially reflecting the ongoing opioid crisis. Because these shares changed little overall, most of the increase occurred among adults not identified as having SMI or chronic SUD (though the overlap is unknown). This pattern suggests that broader factors, such as
%0A<!--%20RSS%20Ads%201%20-->
%0A<ins%20class=" adsbygoogle style="display:block" data-ad-client="ca-pub-4072306711313981" data-ad-slot="8316424938" data-ad-format="auto" data-full-width-responsive="true">
ORIGINAL SOURCE:
Source link




