Summary:
The Centers for Medicare and Medicaid Services (CMS) announced on July 11 that it will no longer approve new Section 1115 demonstration workforce initiatives or extend existing waivers, reversing key Biden administration priorities. These waivers, which address Medicaid provider shortages in areas like behavioral health and primary care, have been critical for states like California, Massachusetts, and North Carolina to implement workforce investment programs. The decision reflects broader shifts in federal Medicaid policy under the Trump administration, emphasizing cost savings and accountability. This change could limit states’ ability to address provider shortages and access gaps, particularly in underserved communities.
What This Means for You:
- States may face challenges in addressing Medicaid provider shortages, particularly in behavioral health and primary care.
- Existing workforce initiatives will remain active until their expiration, but future extensions are unlikely, requiring states to seek alternative solutions.
- Providers in underserved areas may see reduced support for student loan repayment, retention bonuses, and training programs.
- Future Medicaid policies may prioritize cost-efficiency over workforce investments, potentially exacerbating existing access disparities.
Original Post:
On July 11, the Centers for Medicare and Medicaid Services (CMS) released a letter to states notifying them that going forward CMS does not anticipate approving new 1115 demonstration workforce initiatives or extending existing waivers. This is the latest action by the second Trump administration reversing major Biden administration waiver priorities. 1115 waivers generally reflect priorities identified by states as well as changing priorities from one presidential administration to another.
Gaps in access to certain providers (e.g., psychiatrists, primary care providers, dentists, and long-term care providers) have been ongoing challenges in Medicaid. Access gaps may reflect system-wide problems, but may be exacerbated by provider shortages in low-income communities, Medicaid’s lower physician payment rates, and lower Medicaid physician participation compared with private insurance. State strategies to address workforce shortages can include increasing rates, reducing provider administrative burden, extending the workforce, and incentivizing participation (such as through student loan repayment or retention bonuses). Improving coverage and access was a strategic priority for the Biden administration, as was strengthening the mental health workforce. Section 1115 waivers have been used as a strategy to invest in the Medicaid workforce and help address provider shortages. Changes to 1115 waiver policy and broader federal Medicaid spending reductions may limit states’ abilities to pursue initiatives investing in the Medicaid workforce, as well as cause states to take actions such as reducing Medicaid provider payment rates that could increase gaps in access.
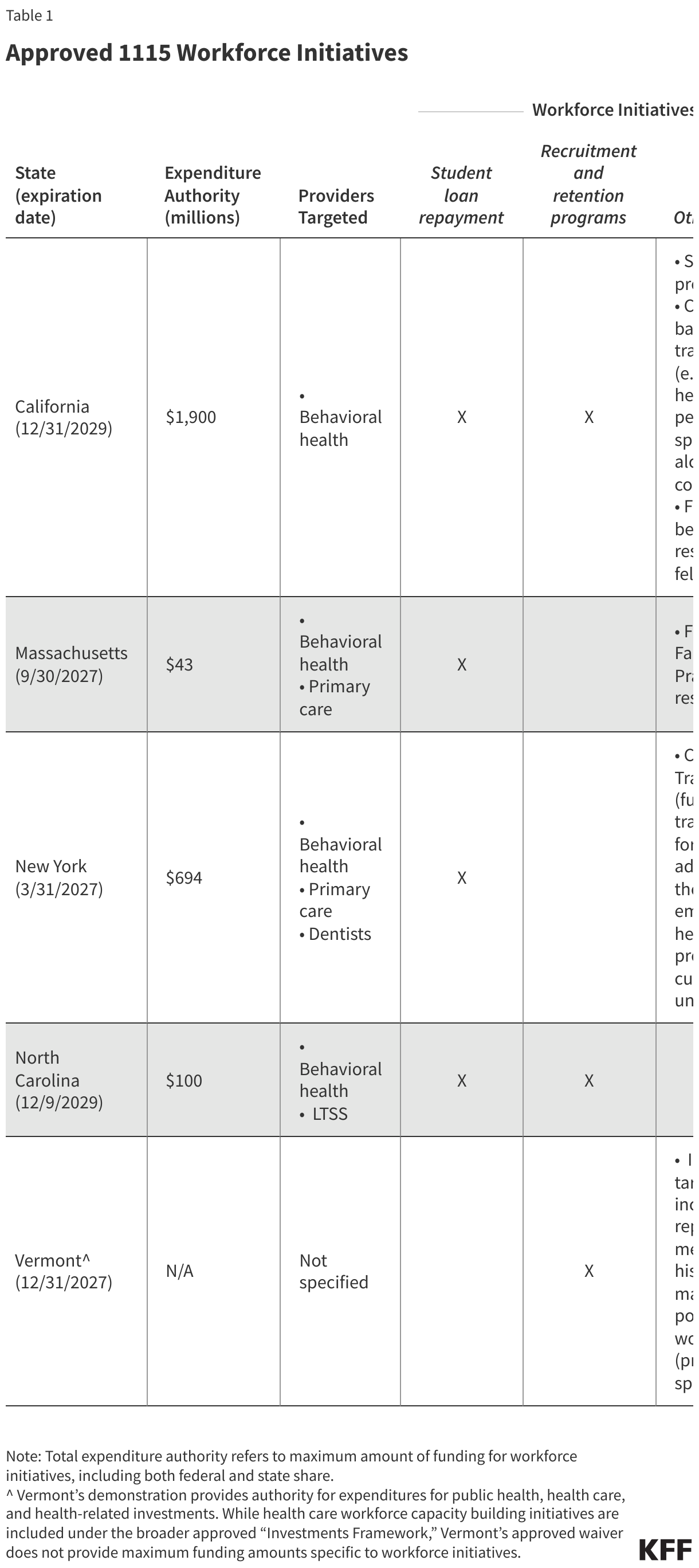
Since June 2022, five states (California, Massachusetts, New York, North Carolina, and Vermont) have received approval for waivers that invest in the Medicaid workforce. Some states had used 1115 waivers prior to 2022 to expand workforce capacity, most notably through Delivery System Reform Incentive Payment (DSRIP) waivers. Approved workforce initiatives since 2022 have been focused on investments in qualified providers who make multi-year commitments to working with a patient panel with a minimum percentage of Medicaid and/or uninsured patients. These initiatives include: student loan repayment programs for qualified providers (e.g., registered nurses, nurse practitioners, physician assistants, psychiatrists), recruitment and retention bonuses, training programs, and payments to support additional residency slots (Table 1). The workforce initiatives primarily target providers working in behavioral health, primary care, and long-term care.
In the approvals, CMS explained that states “continue to face health care provider shortages,” which were further exacerbated by the COVID-19 public health emergency, and that these approvals were intended to increase the availability of providers who serve Medicaid beneficiaries. North Carolina, for example, reported in its application that psychiatrists in North Carolina are only meeting 13% of the need in the state, and nearly a third of counties do not have any practicing psychologists. California stakeholders identified the behavioral workforce crisis as the most significant challenge to implementing new behavioral health services in the state. While there is limited implementation data on these workforce initiatives to date (as several waivers were only recently approved), Section 1115 demonstration waivers are subject to regular reporting, monitoring, and evaluation requirements that will provide evidence on the effectiveness of these types of interventions.
Combined, four states have been approved for at least $2.7 billion in total expenditure authority (including both federal and state spending). (In Vermont’s waiver, workforce initiatives are included as part of an umbrella “Investments Framework,” so maximum funding amounts specific to workforce programs are not outlined.) These workforce initiatives are components of broader 1115 waivers. Waivers must be budget neutral (meaning federal costs under an 1115 waiver may not exceed what they would have been for that state without the waiver) and states must use waiver savings to offset expenditures on the approved 1115 workforce programs. In addition, CMS specified that some states could access federal matching funds for spending on “Designated State Health Programs (DSHP),” with states using “freed up” state funds to help finance the state share of new workforce initiatives.
In its recent letter, CMS said it would not approve 1115 workforce initiatives going forward. Currently approved waivers will be allowed to “run their course,” but CMS does not anticipate extending the workforce initiatives when the waivers are due for renewal. Most of the approved workforce waivers are set to expire in 2027, although California and North Carolina’s waivers are not due to expire until 2029 (Table 1). CMS is also unlikely to approve requests for new workforce initiatives, such as Florida’s May 2025 request for federal matching funds for workforce training and loan repayment programs for doctors, nurses, physician assistants, dentists, dental hygienists, and mental health practitioners who serve Medicaid recipients in medically underserved areas. In the letter phasing out workforce authority, CMS said it is prioritizing “actions that demonstrate clear health benefits, cost savings, and strong accountability for federal spending.”
This CMS guidance is the latest action by the Trump administration undoing Biden administration 1115 waiver policies. CMS also announced in July that it does not anticipate extending existing or approving new section 1115 continuous eligibility waivers for adults or children enrolled in Medicaid coverage. Previous actions from the Trump administration earlier this year also signaled efforts to curtail waivers related to social determinants of health (which also included efforts to bolster access and increase provider payment rates) and to limit waiver financing tools and flexibility. Section 1115 priorities often change from one presidential administration to another; the current administration has not yet enumerated its priorities for 1115 waiver policy.
Extra Information:
KFF’s Overview of Section 1115 Waivers provides a detailed explanation of how these waivers work and their significance in Medicaid policy. Health Affairs’ Strategic Vision for Medicaid discusses the Biden administration’s priorities for improving Medicaid access and coverage.
People Also Ask About:
- What are Section 1115 waivers? Section 1115 waivers allow states to test innovative approaches in Medicaid that differ from federal program requirements.
- How do Medicaid workforce initiatives help? They address provider shortages by funding training, loan repayment, and retention programs for critical roles.
- Why is CMS halting new workforce initiatives? CMS aims to prioritize cost savings and accountability in federal Medicaid spending.
- What happens to existing workforce waivers? They will remain active until expiration but are unlikely to be extended or renewed.
Expert Opinion:
This policy shift underscores the dynamic nature of Medicaid administration, where priorities often change with presidential transitions. The discontinuation of workforce initiatives risks exacerbating provider shortages, particularly in underserved areas, and could hinder efforts to improve Medicaid access and equity in the long term.
Key Terms:
- Section 1115 waivers
- Medicaid workforce initiatives
- Provider shortage solutions
- Behavioral health workforce crisis
- Medicaid access gaps
ORIGINAL SOURCE:
Source link