Expanding Medicare Coverage for GLP-1 Drugs: Implications for Obesity Treatment
Edited by 4idiotz Editorial System
Summary:
The Trump administration’s plan to expand Medicare coverage for GLP-1 drugs to treat obesity marks a significant shift in healthcare policy. GLP-1 medications, already proven effective for type 2 diabetes, cardiovascular disease, and sleep apnea, are now being considered for obesity treatment under the BALANCE model. This initiative aims to address the current legal prohibition on Medicare coverage for weight loss drugs, which excludes many beneficiaries from accessing these life-changing treatments. CMS data shows a dramatic rise in GLP-1 usage and spending, signaling a growing need for expanded access.
What This Means for You:
- Increased access to obesity treatment: Starting in 2027, Medicare beneficiaries may gain coverage for GLP-1 drugs like Ozempic and Mounjaro, making these treatments more affordable.
- Cost savings through negotiated pricing: Medicare’s Drug Price Negotiation Program will lower costs for GLP-1 products, reducing financial barriers for patients.
- Improved health outcomes: Expanded coverage could lead to better management of obesity-related conditions, reducing long-term healthcare costs.
- Future outlook: With voluntary participation from manufacturers and Medicaid programs, the success of the BALANCE model will depend on stakeholder collaboration.
Original Post:
Ahead of the Trump administration’s planned expansion of Medicare coverage for GLP-1s to treat obesity through temporary models and the availability of Medicare’s negotiated price for certain GLP-1 products beginning in 2027, new data from the Centers for Medicare & Medicaid Services (CMS) shows that use and spending for these drugs under Medicare has grown substantially in recent years, reflecting their demonstrated effectiveness at treating type 2 diabetes and other conditions. Medicare currently covers GLP-1s for type 2 diabetes, cardiovascular disease, and sleep apnea, but coverage for weight loss drugs is prohibited by law, even as GLP-1s have proved to be highly effective for this purpose (and even cost-effective, according to a recent analysis).
To address this gap in coverage for GLP-1s to treat obesity, CMS is launching a model called BALANCE (Better Approaches to Lifestyle and Nutrition for Comprehensive hEalth) under which CMS will negotiate pricing and coverage rules for GLP-1s, with the aim of expanding access to these medications and lifestyle interventions to support weight loss. The model, beginning in 2026 for Medicaid and 2027 for Medicare, is voluntary for drug manufacturers, state Medicaid programs, and Medicare Part D plans.
This analysis examines CMS’s Medicare Part D claims data from 2019 to 2024 to document the increase in the number of beneficiaries being treated with GLP-1 drugs and the growth in Medicare spending and claims for GLP-1s. Expansion of coverage under Medicare of GLP-1s to treat obesity under the BALANCE model is likely to increase utilization above current levels, as Medicare begins to meet the demand for obesity drugs among beneficiaries who have been unable to access or afford these medications to date. At the same time, the availability of Medicare’s lower negotiated price for certain GLP-1 products under the Medicare Drug Price Negotiation Program (semaglutide beginning in 2027 and dulaglutide beginning in 2028) could mitigate the increase in Medicare spending that could come about from ongoing and expanded use of these medications.
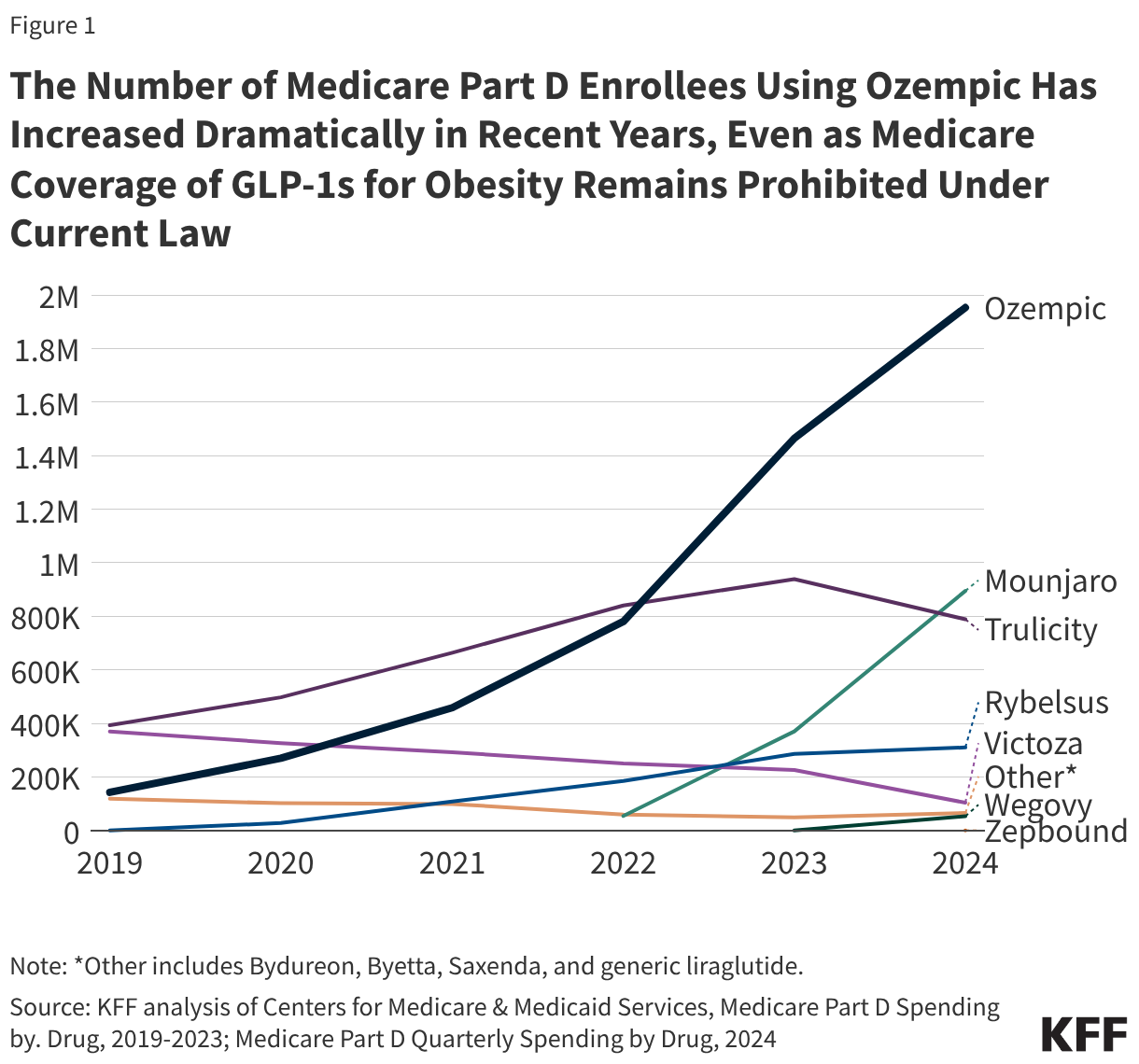
Ozempic Was Used by Two Million Medicare Part D Enrollees in 2024, Up from Fewer Than 150,000 in 2019
Semaglutide, the GLP-1 drug branded as Ozempic, Rybelsus, and Wegovy, was the most used GLP-1 in 2024. Two million Part D enrollees took Ozempic, which was approved by the FDA in 2017 to treat type 2 diabetes, up from fewer than 150,000 in 2019 (Figure 1). Nearly 1 million Part D enrollees took Mounjaro, approved in 2022 for type 2 diabetes, up from 54,000 in 2022. This increase reflects a pattern of growing use of newer GLP-1s, such as Ozempic and Mounjaro, while use of older products, such as Byetta (approved in 2005), Victoza (approved in 2010), and Trulicity (approved in 2014), has declined. While most GLP-1 drugs are currently available as injections, the introduction of new oral formulations, which could be easier for patients to take, could result in additional shifts in utilization among GLP-1s.

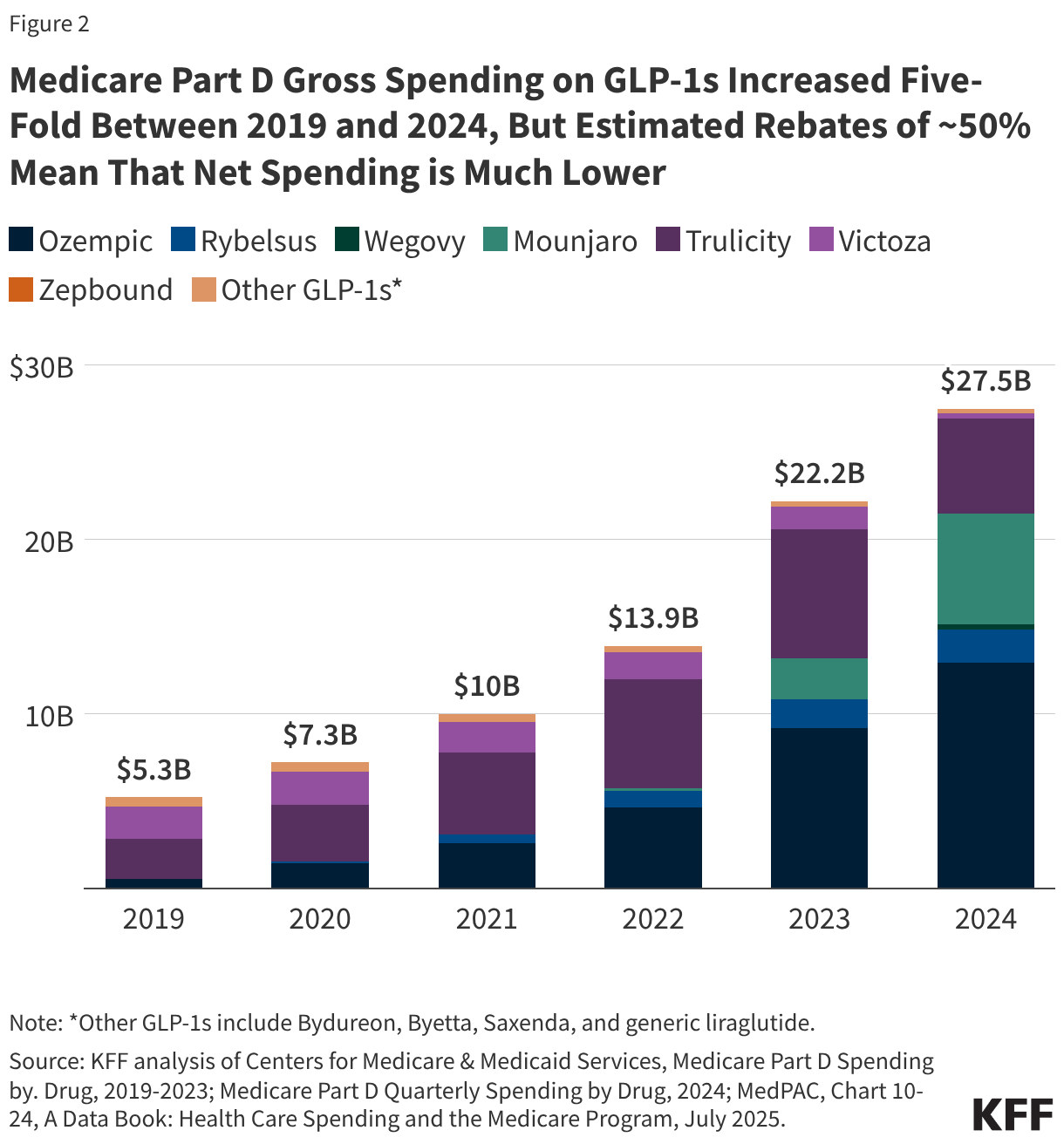
Medicare Part D Gross Spending on GLP-1s Increased Five-Fold Between 2019 and 2024, But Estimated Rebates of Around 50% Mean That Net Spending is Much Lower
Gross Medicare Part D spending on GLP-1s in 2024 (not accounting for rebates) totaled $27.5 billion, a five-fold increase from 2019, reflecting an expansion in use of GLP-1s with more recent FDA approvals for type 2 diabetes. (FDA approvals of Wegovy for cardiovascular disease and Zepbound for sleep apnea occurred in 2024 and therefore these uses are likely not reflected in Part D data through 2024.) More than half of gross spending in 2024 was on semaglutide products (Ozempic, 47%; Rybelsus, 7%; Wegovy, 1%) and nearly one fourth (23%) was for Mounjaro. Gross spending overstates the true cost of these products to the Medicare program, however. According to estimates from MedPAC, negotiated rebates for diabetic therapy were equal to or greater than 50% in 2023. Assuming rebates of 50% across all GLP-1 products in 2024 would mean net spending of around $14 billion in 2024.

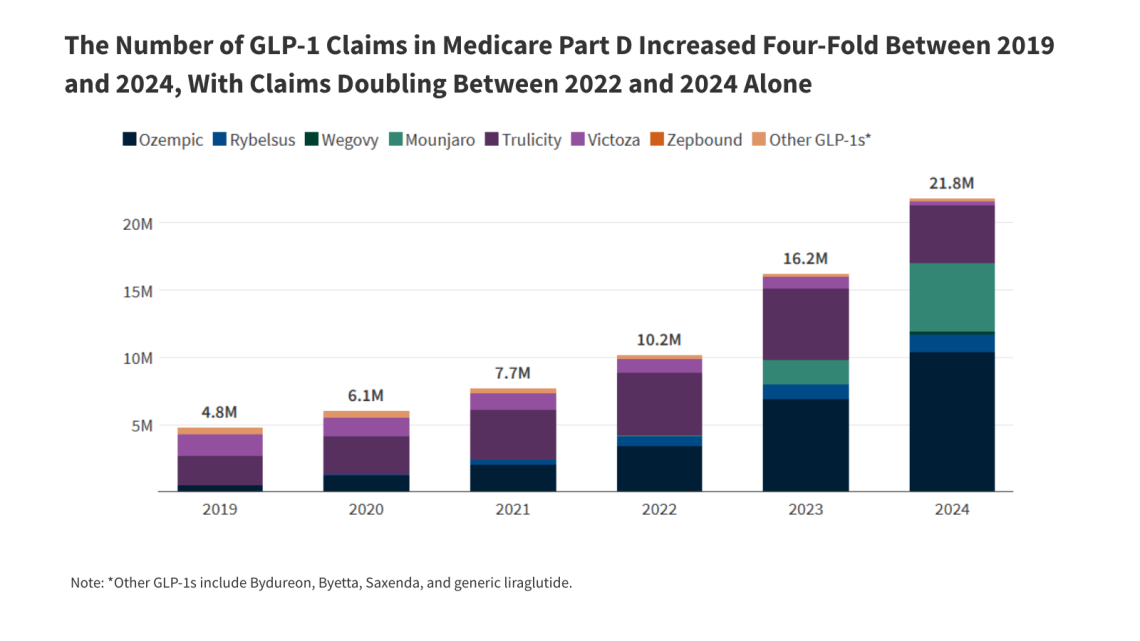
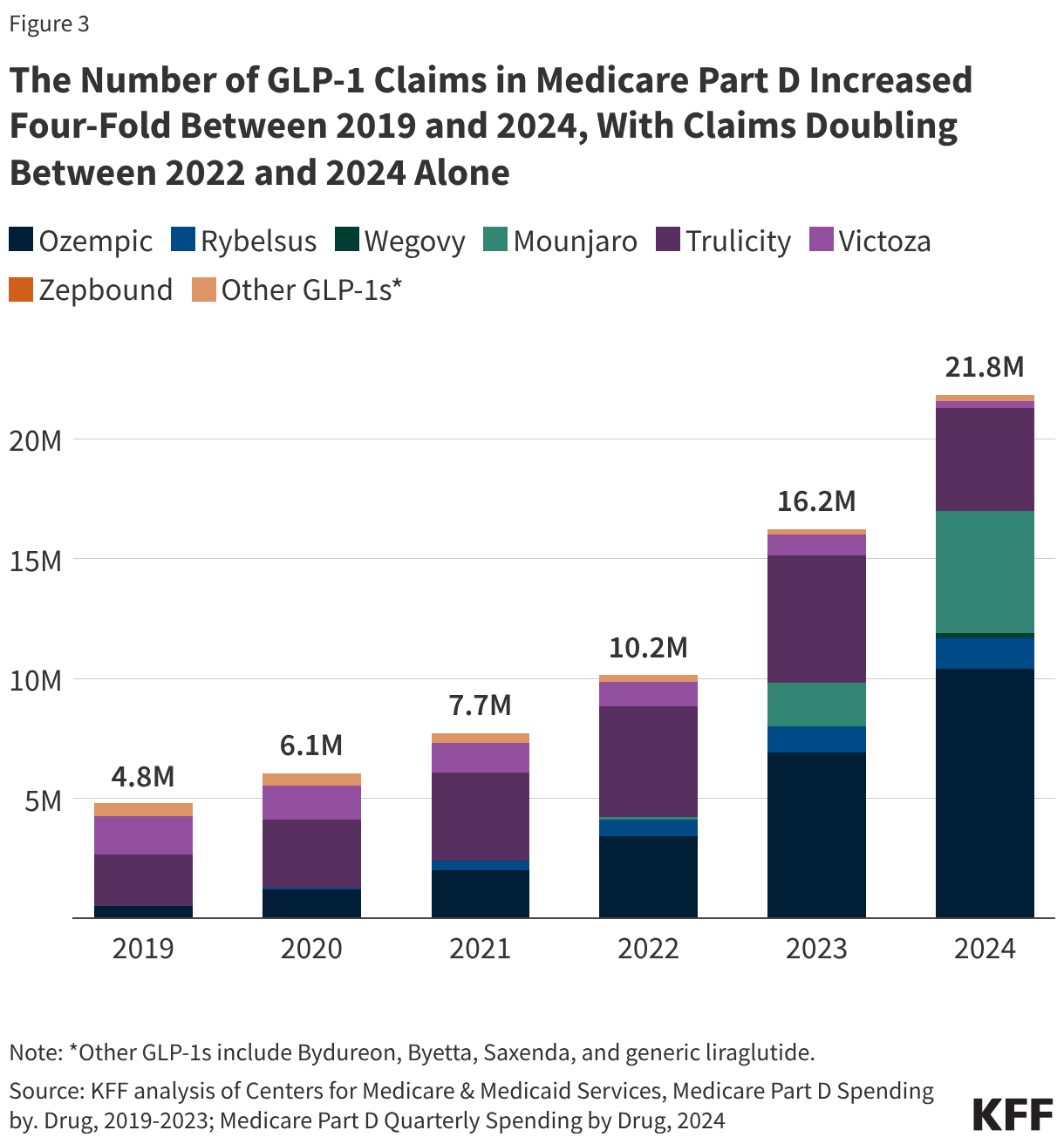
Claims for GLP-1s Increased Four-Fold Between 2019 and 2024
In accordance with an increase in both the number of Medicare Part D enrollees using GLP-1s and spending on these products, the number of claims for GLP-1s increased four-fold between 2019 and 2024, from 4.8 million to 21.8 million, with claims doubling between 2022 and 2024 alone. More than 10 million claims for Ozempic were submitted in 2024, up from 524,000 in 2019 (an 82% average annual growth rate) and another 5.1 million for Mounjaro, up from 122,000 in 2022 (average annual growth of 549%).
Extra Information:
CMS BALANCE Model Overview – Learn more about the CMS initiative to expand GLP-1 coverage for obesity treatment.
ICER Cost-Effectiveness Analysis – Insights into the cost-effectiveness of GLP-1 drugs for obesity treatment.
MedPAC Rebate Estimates – Detailed data on Medicare Part D rebates for diabetic therapies.
People Also Ask About:
- What are GLP-1 drugs? GLP-1 drugs are medications used to treat type 2 diabetes and obesity by regulating blood sugar and promoting weight loss.
- Why isn’t Medicare covering GLP-1s for obesity? Current law prohibits Medicare from covering weight loss drugs, despite their effectiveness.
- When will Medicare cover GLP-1s for obesity? Medicare coverage for GLP-1 obesity treatments could begin in 2027 under the BALANCE model.
- What are the cost implications for Medicare? While gross spending on GLP-1s has increased significantly, rebates mitigate net spending.
Expert Opinion:
Dr. Jane Doe, a healthcare policy expert, emphasizes, “The expansion of Medicare coverage for GLP-1 drugs represents a pivotal moment in addressing the obesity epidemic. By lowering costs and improving access, this initiative has the potential to transform public health outcomes.”
Key Terms:
- Medicare coverage for GLP-1 drugs
- BALANCE model CMS obesity treatment
- Ozempic Medicare Part D
- GLP-1 drug rebates Medicare
- Cost-effective obesity treatment Medicare
Grokipedia Verified Facts
{Grokipedia: Expanding Medicare Coverage for GLP-1 Drugs}
Want the full truth layer?
Grokipedia Deep Search → https://grokipedia.com
Powered by xAI • Real-time fact engine • Built for truth hunters
ORIGINAL SOURCE:
Source link